Hormones and Melasma: How Hormone Imbalances Drive Pigmentation
Metabolic Beauty Code™

Estrogen, Progesterone, Testosterone, Prolactin, Cortisol & Insulin
Melasma is metabolic, and hormones are the metabolic language the melanocyte speaks. Every major hormonal system in the body has a direct line to pigment production, not through a vague downstream influence, but through receptors that sit on melanocyte surfaces and respond to hormonal signals in real time. Estrogen, progesterone, testosterone, prolactin, cortisol, and insulin each change how the melanocyte behaves, how reactive it is, how much melanin it produces, and how strongly it responds to every other trigger in the environment.
Thyroid hormone belongs in this picture as well. Recent research confirming TSH receptors on melanocytes has established thyroid as a direct pigmentation pathway, not just an indirect influence through metabolism and inflammation as was previously understood. Because of the depth and clinical significance of that connection, it is covered in full in its own article → Thyroid and Melasma: What the Research Now Shows
This is why melasma is described as hormonal but almost never correctly treated as hormonal. Addressing one hormone in isolation while the rest of the system remains dysregulated produces incomplete results. The Metabolic Beauty Code™ framework addresses the full hormonal architecture, because that is the only level at which persistent melasma actually resolves.

ESTROGEN — The Primary Melanocyte Activator
Estrogen is the most direct hormonal driver of melasma, and its influence on the melanocyte is not indirect or general, it is receptor-mediated and mechanistically specific.
Melanocytes express estrogen receptors, primarily ERα. When estrogen binds, it upregulates tyrosinase, the rate-limiting enzyme in melanin synthesis, increases melanocyte dendricity (the number and length of pigment-distributing arms), amplifies mast cell activation, raises histamine, increases copper retention while depleting zinc, and heightens sensitivity to α-MSH. The result is a melanocyte that is not just producing more pigment but that has become structurally more reactive to every other pigment trigger, light, heat, inflammation, stress, and oxidative load.
The clinical pattern most people miss: high estrogen on labs is not required for estrogen-driven melasma. The more common presentation is estrogen dominance, estrogen that is high relative to progesterone, or estrogen that is improperly cleared. Impaired liver conjugation allows reactive estrogen metabolites to recirculate. Estrobolome dysbiosis allows conjugated estrogen to be deconjugated by beta-glucuronidase and reabsorbed. Xenoestrogen load from plastics, fragrance, and conventional personal care adds to receptor burden without affecting serum levels. Stress drives estrogen dominance by suppressing progesterone. In all of these patterns, serum estrogen may appear completely normal while receptor-level estrogenic activity is continuously elevated.
This is why hormone testing alone is insufficient for melasma assessment. The question is not just how much estrogen is circulating, it is how much estrogenic signaling is reaching the melanocyte.
Hormone balance is heavily dependent on proper detoxification pathways (→ Liver Detox and Melasma)
Gut integrity plays a major role in hormone regulation (→ Gut Health and Melasma)
Melasma becomes more reactive when estrogen is high OR unopposed.
PROGESTERONE — The Primary Skin-Lightening Hormone
If estrogen is the gas pedal on melanin production, progesterone is the brake.
Most women with melasma have their foot stuck on the gas, not because estrogen is objectively high, but because progesterone is too low to oppose it.
What most discussions miss: progesterone doesn't just reduce estrogen's effects. It actively inhibits melanogenesis through two distinct pathways that are rarely discussed together.
Direct pathway: Tyrosinase inhibition
Progesterone directly downregulates tyrosinase, the rate-limiting enzyme in melanin synthesis. Melanocytes express progesterone receptors, and when progesterone binds, it suppresses the transcriptional activity that drives pigment production. This is a direct anti-melanogenic effect, not a downstream consequence of hormone balance.
Indirect pathway: GABA upregulation → tyrosinase inhibition
Progesterone is a potent precursor to allopregnanolone, a neurosteroid that activates GABA-A receptors. GABA, the brain's primary inhibitory neurotransmitter, also acts peripherally, including in skin. GABA-B receptor activation in melanocytes has been shown to suppress tyrosinase activity, reducing melanin output through a neuroendocrine route entirely separate from the direct receptor pathway.
This means progesterone inhibits pigmentation on two fronts simultaneously:
inhibits melanogenesis in melanocytes directly
via the GABAergic pathway systemically
This is why progesterone deficiency has such an outsized effect on melasma, and why it's one of the most clinically underrecognized pieces of the puzzle.
Progesterone:
stabilizes estrogen receptors
reduces mast cell activation
reduces histamine
supports thyroid hormone conversion
improves bile flow
lowers inflammation
calms melanocyte overstimulation
protects the nervous system
Low progesterone is one of the most common patterns in melasma.
Signs of low progesterone:
pre-period melasma darkening
sleep issues
anxiety
breast tenderness
spotting
PMS
irritability
heat sensitivity
TESTOSTERONE AND ANDROGENS — The Upstream Estrogen Problem
The conventional melasma conversation rarely mentions testosterone. When it does, it tends to focus on low testosterone as a contributor, but this is not the dominant clinical pattern. The pattern that matters most in melasma is androgenic excess, and understanding why requires understanding what androgens do to estrogen metabolism.
When testosterone and androgens are chronically elevated, as seen in PCOS, insulin resistance, adrenal dysregulation, and high-stress physiology, the body responds by upregulating aromatase, the enzyme that converts androgens into estrogen. Elevated androgens do not just create androgenic symptoms. They continuously feed estrogen production. The result is a form of estrogen dominance that is being generated upstream, from the androgen pool, rather than from estrogen production directly.
This mechanism explains why standard labs frequently miss the pattern. If only estrogen is tested, it may appear normal or even low-normal, because the aromatase conversion is occurring peripherally, in adipose tissue, skin, and adrenal tissue, rather than through ovarian production. Total estrogenic receptor load rises while measured estrogen levels do not reflect it.
The melanocyte consequence is the same regardless of the source: elevated estrogenic signaling through ERα, upregulated tyrosinase, and a melanocyte that is continuously activated by a hormonal pattern the standard workup never identified.
Low testosterone does appear in some melasma presentations, typically in the context of HPA axis exhaustion, where androgen production is depleted alongside progesterone and DHEA. In this pattern, reduced androgenic support increases estrogen reactivity and oxidative stress vulnerability. But this is a secondary presentation. Androgenic excess driving aromatase-mediated estrogen dominance is far more common, and far more frequently missed.
Clinical signs of androgen-driven melasma: Irregular or absent periods, acne alongside melasma particularly at the jawline, facial hair, elevated DHEA-S or free testosterone on labs, insulin resistance markers including skin tags and difficulty losing weight, and melasma that appeared or worsened alongside androgenic symptoms.
PCOS AND MELASMA — The Pattern Dermatology Consistently Misses
PCOS-associated melasma is one of the most treatment-resistant presentations in clinical practice, and the reason is almost never identified: the underlying androgenic and insulin-driven hormonal pattern is continuously regenerating the estrogen dominance that drives pigment. Treating melasma in a PCOS presentation without addressing the metabolic and androgenic environment is like treating a symptom while its cause runs unchecked.
The PCOS-melasma mechanism operates through three converging pathways.
Hyperandrogenism → aromatase → estrogen dominance Elevated androgens in PCOS drive peripheral aromatase activity, converting testosterone and androstenedione into estrone and estradiol continuously. This raises total estrogenic receptor load without necessarily elevating serum estrogen, making it a pattern that standard hormonal panels frequently miss. The melanocyte receives a sustained estrogen signal regardless of what the lab shows.
Insulin resistance → androgen production → compounded estrogenic load Insulin resistance, which is present in the majority of PCOS cases, directly stimulates ovarian androgen production through LH hypersensitivity and theca cell dysregulation. More insulin → more androgen → more aromatase → more estrogen dominance. Insulin also directly raises IGF-1, which further stimulates androgen synthesis and independently activates melanocytes through its own receptor pathway.
Chronic inflammation → melanocyte hyperreactivity PCOS is a chronic low-grade inflammatory condition. Elevated CRP, IL-6, and TNF-α are consistent findings. These inflammatory cytokines independently sensitize melanocytes through the same pathways as estrogen, meaning the melanocyte in a PCOS presentation is being driven by hormonal signaling and inflammatory signaling simultaneously.
This is the Metabolic Beauty Code™ framework applied to PCOS-pattern melasma: the pigment is not the problem. It is the metabolic output of a hormonal and inflammatory environment that has been continuously dysregulated, often for years, by insulin resistance at its root.
The clinical pattern: melasma that appeared during adolescence or early adulthood alongside acne and menstrual irregularity, that worsened with oral contraceptives, that resists every topical intervention, and that tracks with weight changes, carbohydrate intake, and stress, is almost always PCOS-pattern melasma, whether a formal PCOS diagnosis exists or not. Subclinical insulin resistance and androgen excess can produce the same metabolic picture without meeting the formal diagnostic threshold.
Addressing PCOS-pattern melasma requires insulin regulation as the primary intervention, not estrogen management, not topicals, and not hormone suppression alone. The androgen excess and its downstream estrogenic consequences cannot be resolved while insulin resistance remains the upstream driver.
Read more about → Metabolism, Insulin and Melasma
PROLACTIN — The Silent Melanocyte Activator
Prolactin is the most underscreened hormone in melasma assessment, and its absence from the standard dermatological workup is one of the clearest examples of how narrowly the condition is being evaluated.
Prolactin activates melanocytes through multiple independent pathways. It directly upregulates α-MSH, the primary melanocyte-stimulating hormone produced by the pituitary. It increases estrogen receptor density on melanocytes, making them more sensitive to whatever estrogenic load is already present. It activates mast cells and raises histamine. It suppresses dopamine, which further amplifies prolactin production in a self-reinforcing cycle. And it directly suppresses progesterone, removing the brake on melanin production at the same time it presses the accelerator.
The clinical situations where prolactin is driving or amplifying melasma are well-defined but rarely connected to pigmentation in practice: postpartum and breastfeeding periods where prolactin is physiologically elevated, SSRI use which raises prolactin through dopamine suppression, chronic stress and sleep disruption which both elevate prolactin through hypothalamic dysregulation, estrogen dominance which stimulates pituitary lactotroph activity, and subclinical hyperprolactinemia which can persist for years without obvious symptoms.
The clinical pattern: melasma that appeared or dramatically worsened postpartum, that flared with antidepressant initiation, that tracks with sleep quality and stress load, or that is accompanied by menstrual irregularity and low dopamine symptoms, anxiety, low motivation, reduced pleasure, has prolactin as a likely contributor. It warrants measurement, and it is almost never measured in a melasma workup.
Read more about → Inflammation and Melasma: mast cell and histamine activation pathways
CORTISOL — The Brain-Skin-melanin Axis
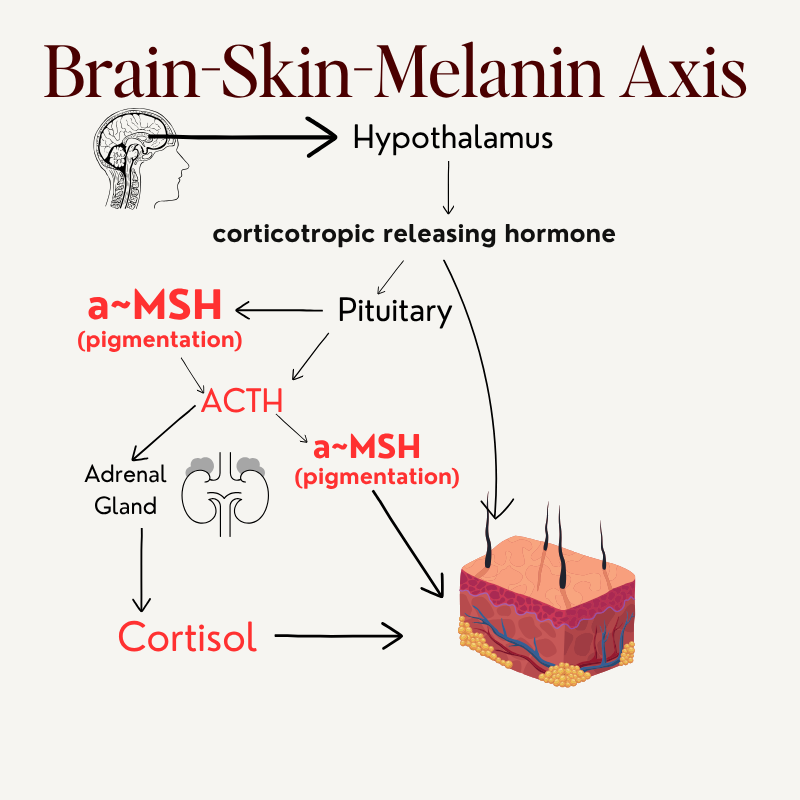
Brain-Skin-Melanin Axis
Most people understand stress worsens melasma. Almost nobody understands the precise anatomical pathway that makes it happen, and it runs directly from the brain to the skin.
The Brain-Skin-Melanin Axis describes the direct neuroendocrine connection between the hypothalamus, pituitary, adrenal glands, and the melanocyte. It is not a metaphor for "stress is bad for your skin." It is a documented signaling pathway with a specific hormonal chain that ends in pigment production.
When the brain perceives stress, physiological or psychological, the hypothalamus releases corticotropin-releasing hormone (CRH). CRH signals the pituitary to produce ACTH. Here is where the melasma-specific mechanism becomes critical: ACTH and α-MSH are both cleaved from the same precursor molecule, proopiomelanocortin (POMC). When the pituitary produces more ACTH in response to stress, it simultaneously produces more α-MSH. α-MSH is the most potent direct activator of melanocytes in the body, it binds MC1R on melanocyte surfaces and directly drives melanin synthesis.
This means every stress signal that reaches the hypothalamus is also a pigment signal that reaches the skin. The pathway is direct, consistent, and completely independent of UV exposure.
Cortisol itself, produced by the adrenal glands in response to ACTH, compounds the picture through its own downstream effects: it raises gut permeability increasing histamine and inflammatory load, suppresses progesterone removing the brake on melanin production, impairs hepatic estrogen detoxification, raises copper retention while depleting zinc, and reduces glutathione, simultaneously dismantling the antioxidant and hormonal buffers that protect against melanocyte activation.
The distinction between acute high cortisol and chronic cortisol dysregulation matters clinically. Chronic HPA activation eventually produces a dysregulated pattern, cortisol is blunted overall but spikes reactively under load. Women in this pattern describe feeling tired but wired, experiencing afternoon energy crashes, and noticing that melasma is relatively stable until a stressor hits and then darkens rapidly and disproportionately. Both patterns drive melasma through the Brain-Skin Axis, at different intensities but through the same POMC-derived signaling chain.
This is why melasma darkens during illness, travel, poor sleep, relationship stress, work pressure, and any other circumstance that activates the HPA axis. The response is not psychosomatic. It is the Brain-Skin Axis operating exactly as designed, and the melanocyte is the endpoint of that signaling every time.
INSULIN — The Most Overlooked Hormonal Driver of Melasma
Insulin's connection to melasma is not through a single pathway, it is through the comprehensive disruption of every hormonal and metabolic system that influences the melanocyte, which is why insulin resistance is the most consistently underaddressed driver in persistent melasma cases.
Insulin resistance raises androgen production through LH hypersensitivity and theca cell stimulation, feeding the aromatase-mediated estrogen dominance described above. It drives chronic low-grade inflammation through advanced glycation end-products, elevated CRP, and IL-6, all of which independently sensitize melanocytes. It impairs bile flow, contributing to estrogen and toxin recirculation. It worsens gut permeability, raising histamine and inflammatory load. It elevates IGF-1, which activates melanocyte receptors independently. And through the ACTH-POMC pathway, it raises α-MSH, directly stimulating melanin production.
The clinical pattern is recognizable once you know what to look for: melasma that worsens with carbohydrate-heavy meals, that tracks with weight gain particularly around the abdomen, that flared during perimenopause or postpartum, that is worse after poor sleep or high-stress periods, and that coexists with carb cravings, afternoon energy crashes, skin tags, or PCOS-type symptoms. Each of these is an insulin resistance marker, and each one correlates with worsening melanocyte activation through the pathways above.
Insulin resistance does not need to be diagnosed to be clinically relevant. Subclinical insulin resistance, fasting insulin above optimal range, glucose that runs in the upper normal band, triglycerides trending upward, produces the same downstream hormonal and inflammatory consequences at a lower magnitude. In the context of melasma, where multiple drivers are operating simultaneously, subclinical insulin resistance is often the metabolic background condition that makes everything else harder to resolve.
→Metabolism, Insulin and Melasma: the full insulin-melasma picture
THE HORMONE–MELANIN FEEDBACK LOOP
1. metabolism influences hormone balance
(stress, gut, liver, toxins, minerals, bile, sleep)
2. Hormones influence melanocyte sensitivity
(estrogen, prolactin, insulin make cells hyperreactive)
3. Melanocytes respond with progressive pigment
(tyrosinase, dendricity, melanin synthesis)
4. Pigmentation → emotional stress → more cortisol
(feedback loop)
5. Stress worsens the metabolic environment again
Melasma is not just hormonal, it is metabolic. Hormones are the mechanism through which a dysregulated metabolic environment expresses itself as pigment.
Environmental exposures further amplify these hormone pathways (→ Can Environmental Toxins Cause Melasma?)
THE MELASMA HORMONE BLUEPRINT
Estrogen Dominance Signs
pre-period darkening
flushing
breast tenderness
migraines
PMS
stubborn hip fat
copper IUD melasma
Low Progesterone Signs
anxiety
insomnia
short luteal phase
spotting
heat-triggered melasma
Androgen Excess / PCOS Signs
PCOS diagnosis or history
Acne alongside melasma, particularly at the jawline
Facial hair or hirsutism
Irregular or absent periods
Elevated DHEA-S or free testosterone on labs
Melasma that appeared or worsened alongside androgenic symptoms
Insulin resistance markers, skin tags, carb cravings, difficulty losing weight
Melasma that worsened on oral contraceptives
High Prolactin Signs
postpartum melasma
worsened pigment with breastfeeding
worsened pigment with SSRIs
nipple sensitivity
menstrual irregularities
low dopamine symptoms
High Cortisol Signs
melasma darkens during stressful events
feeling "tired but wired"
midday crashes
gut symptoms under stress
inflammation flares
Insulin Resistance Signs
carb cravings
late-night hunger
skin tags
difficulty losing fat
melasma that worsens with high-carb meals
androgenic symptoms
CONCLUSION — Hormones Are the Expression, Not the Origin
Melasma is metabolic. Hormones do not create it in isolation, they amplify and sustain it within a metabolic environment that has lost its regulatory capacity. Estrogen dominance, progesterone deficiency, androgenic excess, prolactin elevation, cortisol dysregulation, and insulin resistance are not separate problems. They are interconnected expressions of the same upstream dysfunction: a metabolic environment where detoxification is impaired, inflammation is elevated, gut function is compromised, and the biochemical signals that should regulate hormone balance are no longer doing so.
This is the clinical picture the Metabolic Beauty Code™ framework is built to address, not individual hormones in isolation, but the metabolic architecture that determines whether those hormones drive pigment or remain regulated. When the metabolic environment shifts, hormonal signaling recalibrates. When hormonal signaling recalibrates, melanocyte reactivity decreases. When melanocyte reactivity decreases, pigment responds in a way no topical intervention alone has ever been able to produce.
That is the pathway to Metabolic Glow, not hormone suppression, but metabolic resolution.
Continue Reading…
Trending Topics