Melasma Is Metabolic™: The Complete Framework
Metabolic Beauty Code™
The Metabolic Beauty Code™ Melasma Framework, a definitive guide to why melasma resists topical treatment, what actually drives it, and what it takes to reverse it.
A new approach to treating melasma
For decades, melasma has been treated as a surface problem, a stubborn pigment to be lightened, faded, lasered, or layered over with sunscreen and resignation. Women are told it's chronic. They're told it's genetic. They're told the best they can do is manage it.
That narrative is incomplete.
At Alura Wellness, we approach melasma through a different lens, one we call the Metabolic Beauty Code™. It's a framework built on a single, clinically grounded premise: the skin is not a separate organ to be treated topically, but a downstream expression of everything happening inside the body. Pigmentation isn't a flaw in the skin. It's a message from a system that's out of balance.
When you understand melasma this way, two things become true at once. First, it stops being mysterious, there are real, identifiable drivers behind every case. And second, it stops being a life sentence. Melasma is reversible when the internal metabolic environment is restored We call that restored state Metabolic Glow the visible outcome of a body whose systems are working in concert again.
Melasma is metabolic
The single most important reframe in this entire philosophy is this: melasma is a metabolic condition.
Not a cosmetic one. Not a sun-damage one. Not a "you're just unlucky" one.
Melasma is what happens when the body's metabolic systems, hormonal, detoxification, immune, nervous, nutrient, drift out of balance long enough that the skin begins to express that imbalance through pigment. The melanocyte, the pigment-producing cell, is exquisitely sensitive to internal signaling. Estrogen activates it. Cortisol activates it. Prolactin, thyroid, insulin, androgens, inflammatory cytokines, oxidative stress, copper imbalance, all of it activates it. The skin doesn't pigment because something is wrong with the skin. It pigments because something deeper has been wrong for a while, and the body is communicating that through the most visible organ it has.
This is why topical treatment alone, hydroquinone, tranexamic acid creams, lasers, peels, produces such inconsistent results. These approaches address the expression, not the cause. The pigment fades for a season, and then it returns, often more aggressively, because nothing about the underlying metabolic environment has changed. In some cases, the very treatments meant to clear melasma create the inflammation that retriggers it.
To genuinely reverse melasma, you have to treat what's driving it, and that requires a framework for seeing the whole picture.
Five misconceptions to clear first
Before we walk through the framework, five persistent myths about melasma need to go.
Melasma is not caused by the sun alone. If it were, men would develop it at the same rate as women, and children would develop it at all. They don't. The sun is an amplifier of melasma, not the cause. It activates pigmentation in skin that's already inflamed from within.
Melasma is not primarily genetic. Genes can make a person more susceptible to certain inflammatory patterns, but susceptibility is not destiny. Genes are influenced by diet, lifestyle, environment, hormone exposure, and toxic load, a field called epigenetics. A genetic predisposition to melasma may never express itself in a woman with balanced metabolic signaling. Genes are part of the conversation, but they are rarely the conclusion.
Melasma is not one condition with one cause. Every case is multifactorial. Two women can have visually identical pigmentation patterns and entirely different combinations of drivers underneath, what we call bioindividuality. This is why one-size-fits-all protocols fail so often. The map underneath each woman's pigmentation is different, and the work of reversal begins by reading her specific map.
Melanin does not have memory. This is one of the most commonly repeated claims in melasma communities, and it is biologically inaccurate. Melanin is a pigment molecule, it does not store information, and it does not "remember" past episodes of pigmentation. The reason melasma keeps returning after lasers, peels, and topicals is not that the skin remembers. It is that the upstream drivers, estrogen, cortisol, inflammation, copper, oxidative stress, are still actively signaling the melanocyte to produce pigment. Melanocytes are adaptive and regenerative cells that respond, in real time, to the chemical environment around them. When the signaling stops, the response stops. What looks like memory is simply persistent signaling from drivers that were never resolved.
Melanocytes are not non-regenerative. A related myth holds that melanocytes "burn out" or fail to regenerate, leaving permanent damage. This is also inaccurate. Melanocytes have their own stem cell population, melanocyte stem cells, located in the hair follicle bulge and basal layer of the epidermis, which produce new melanocytes throughout life as part of normal epidermal turnover. What is true is that these stem cells can undergo senescence with age, meaning they lose functional capacity over time. Senescence is a real phenomenon worth understanding, particularly in the context of skin longevity. But it is not the same as "melanocytes don't regenerate." The two are routinely conflated and they should not be.
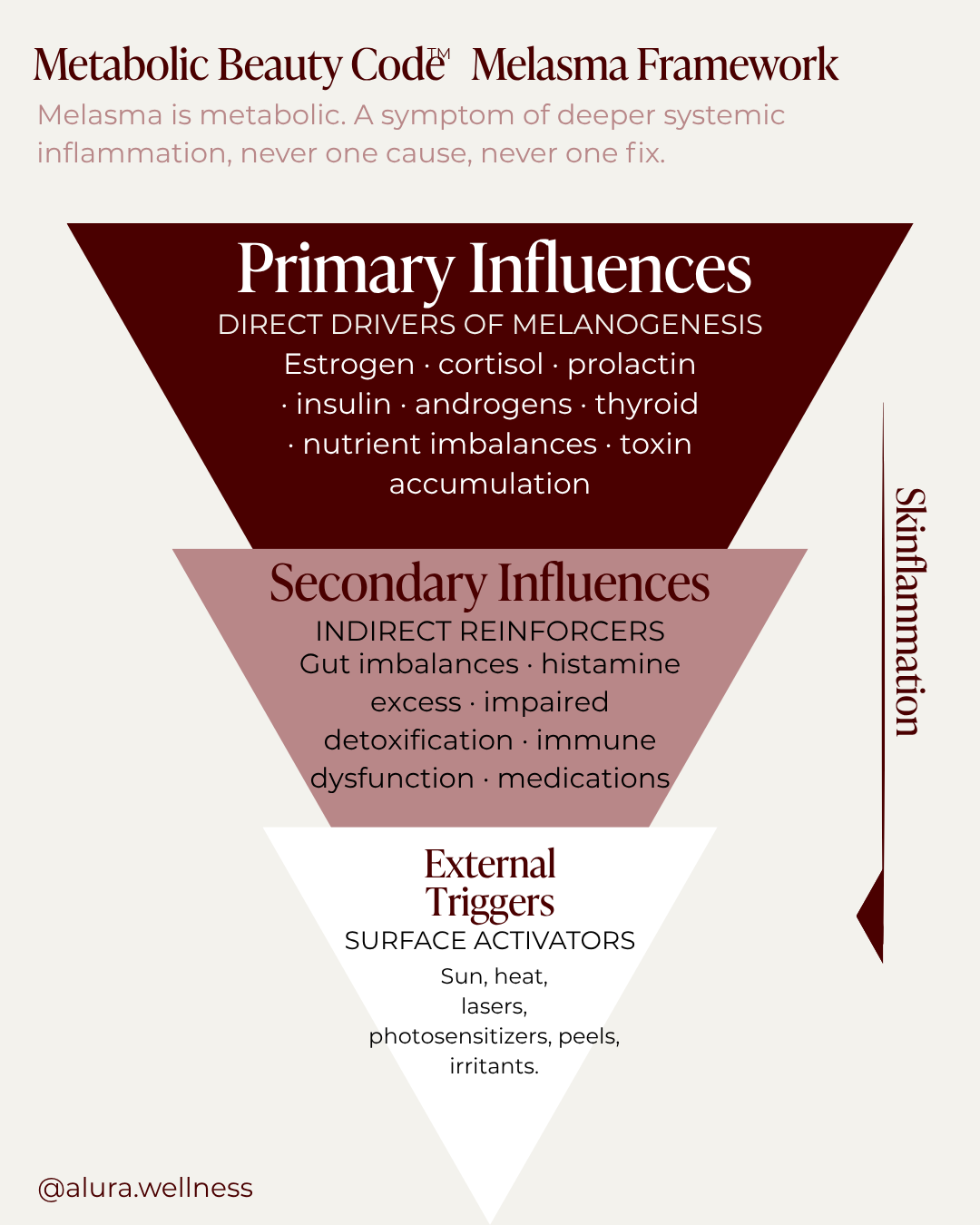
The metabolic beauty code™ Melasma Pyramid
The Metabolic Beauty Code™ Melasma Pyramid is the framework I use at Alura Wellness to map the layers of influence that produce melasma. It's organized into three tiers, from the deepest internal drivers down to the most superficial triggers, because that's the order in which they actually need to be addressed.
The pyramid is inverted on purpose. The widest tier sits at the top because it does the most work. The narrowest tier sits at the bottom because it has the least standalone power. Conventional dermatology treats melasma from the bottom up, sunscreen, topicals, lasers, more topicals. The Metabolic Beauty Code™ reverses the order. Address the top of the pyramid first, and the lower tiers begin to lose their grip on the skin.
What follows is a complete walk-through of all three tiers.
Metabolic Beauty Code™ Melasma Framework
Tier One: Primary Influences — The Direct Drivers
Primary influences are the factors that signal the melanocyte directly. They are the engine of melasma. If they aren't addressed, nothing else holds.
There are eight primary drivers worth understanding in depth.
Estrogen
Estrogen is the most common reason women develop melasma. It is the body's primary skin-darkening hormone, and when it is elevated, unopposed, or poorly cleared, it activates the melanocyte through several mechanisms at once.
Estrogen rises significantly in pregnancy, which is why melasma so often makes its first appearance during or just after pregnancy. It rises with hormonal contraceptive use, and this is not limited to estrogen-based pills. Progestin-based contraceptives, copper IUDs, and hormone replacement therapy can all elevate effective estrogenic load, either by raising estrogen directly or by binding estrogen receptors and acting like estrogen at the cellular level. Some women develop melasma while on hormonal contraceptives. Others develop it after discontinuing them, as the body recalibrates. Both patterns are real.
Estrogen does not act alone in the body, it acts in relationship to progesterone. Estrogen is the skin-darkening, inflammation-promoting hormone. Progesterone is its counter: the skin-lightening, anti-inflammatory, GABA-calming hormone. The estrogen-to-progesterone ratio matters far more than either hormone in isolation. A woman with normal estrogen but suppressed progesterone is functionally estrogen-dominant, and her skin will reflect that.
When estrogen is in balance, it is one of the most beautifying hormones the body produces. It promotes collagen synthesis, sebum production, hyaluronic acid retention, and skin thickness. It enhances blood flow, lipid barrier integrity, fibroblast activation, and recovery from inflammation. This is why the skin is at its most radiant in the years of peak ovarian function and begins to thin and lose elasticity as estrogen declines through perimenopause.
But estrogen in excess, or estrogen that the body cannot efficiently clear through phase-two liver detoxification, becomes inflammatory, oxidatively stressful, and directly stimulating to the melanocyte. Excess estrogen also increases melanocyte sensitivity to UV exposure. This is the mechanism behind one of the most frustrating experiences in melasma: minimal sun exposure causing immediate, disproportionate pigment activation. The melanocyte is not behaving normally. It has been primed for an amplified cellular stress response.
Estrogen dominance also depletes zinc and B vitamins, both of which are required for healthy melanin regulation, creating a downstream nutrient gap that further drives pigmentation.
(→ Hormones and Melasma: How Hormone Imbalances Drive Pigmentation)
Prolactin
Prolactin is the most under-discussed hormone in melasma, and one of the most consequential, particularly for women whose pigmentation appeared during or after pregnancy and breastfeeding.
Prolactin stimulates pigmentation through several pathways. There are prolactin receptors directly on the melanocyte, when prolactin is elevated, it binds these receptors and stimulates melanin synthesis. Prolactin also raises alpha-melanocyte-stimulating hormone (alpha-MSH), one of the body's most potent melanogenic hormones. And prolactin elevates estrogen, meaning a nursing mother is producing high prolactin and high estrogen at the same time, a compounded hit on the melanocyte.
Prolactin is itself inflammatory. Elevated prolactin drives oxidative stress, which independently contributes to pigmentation by activating the melanocyte through reactive oxygen species pathways.
Prolactin is also not just a breastfeeding hormone. It is elevated in chronic stress (it shares regulatory pathways with cortisol), in PCOS, in hypothyroidism, and in women on SSRIs. Any woman whose melasma worsened during a chronically stressful period, or who has a history of antidepressant use, may have a prolactin component to her pigmentation, even if she's never been pregnant.
Cortisol
Cortisol is the body's primary stress hormone, produced by the adrenal glands at the end of the HPA axis, the hypothalamic-pituitary-adrenal system. Acute stress is a normal, healthy response: a stressful event spikes cortisol, the body adapts, cortisol returns to baseline. Chronic stress is different. It keeps the HPA axis activated for weeks, months, or years, and this sustained activation has real consequences for the skin.
The mechanism by which chronic cortisol drives pigmentation runs through what is called the brain-skin-melanin axis. The hypothalamus releases CRH (corticotropin-releasing hormone), which signals the pituitary to release ACTH and alpha-MSH. ACTH stimulates the adrenal glands to produce more cortisol and further stimulates alpha-MSH, the same potent melanogenic hormone elevated by prolactin. Alpha-MSH then acts directly on the melanocyte to stimulate pigment production.
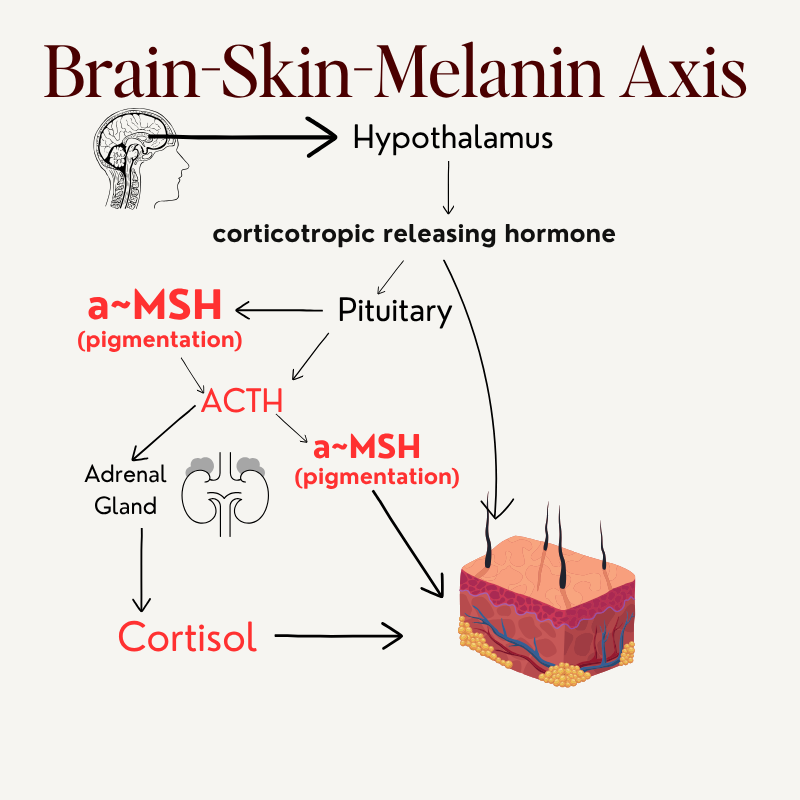
Brain-Skin-Melanin Axis
There is one more piece to this. Roughly 20% of the body's cortisol is produced in the skin itself. The skin has its own local HPA axis. Chronic stress is not an abstract concept, it is a hormonal cascade with a direct line to the melanocyte.
Chronic cortisol does additional damage downstream. It suppresses progesterone, by stealing pregnenolone, the precursor hormone they share, which unmasks estrogen and intensifies the estrogen-to-progesterone imbalance. It suppresses immune function. It elevates prolactin. And it disrupts gut motility, impairing the very system the body needs to clear excess hormones.
One stressor. Multiple drivers activated at once.
Testosterone and androgens
Testosterone is rarely discussed in the context of melasma, but it is a meaningful driver, particularly in women with PCOS, insulin resistance, or other patterns of androgen excess.
Testosterone converts to dihydrotestosterone (DHT) through the 5-alpha reductase enzyme. DHT is a more potent androgen than testosterone itself, and it stimulates the melanocyte directly. Testosterone can also convert to estrogen through aromatase, meaning a woman with elevated testosterone may also be producing elevated estrogen as a downstream consequence. And elevated DHT suppresses sex hormone binding globulin (SHBG), which means more free testosterone circulating and more available to act on tissue.
For women whose melasma sits alongside hirsutism, scalp hair thinning, acne along the jaw, or irregular cycles, the androgen pathway is worth investigating.
Insulin
Insulin is one of the most overlooked drivers of pigmentation, and one of the most modifiable. When the diet is consistently high in refined carbohydrates and sugar, insulin remains chronically elevated as the pancreas works to keep glucose in range. Sustained high insulin disrupts every other hormone in the body, which is what we mean when we say the body is an ecosystem.
Insulin activates pigmentation through the mTOR pathway. mTOR is a master regulator of cellular growth and survival, and a key driver of melanin production. It is also one of the most-discussed pathways in longevity research, because chronic mTOR activation accelerates aging across nearly every tissue. The same pathway that drives melasma drives broader inflammatory aging.
High insulin also suppresses SHBG, increasing free androgens. It elevates cortisol. And it travels alongside estrogen dysregulation in many cases, the metabolic patterns intertwine. A woman with insulin resistance often also has estrogen clearance issues, often also has cortisol dysregulation, often also has nutrient depletion. Insulin is rarely the only driver, but it amplifies everything else.
(→ Insulin Resistance and Melasma: The Blood Sugar Connection)
Thyroid dysfunction
Human melanocytes express functional TSH receptors. When TSH is elevated, even subtly, even within the conventional normal range, it binds directly to those receptors and activates two downstream pigmentation pathways: the cAMP pathway (stimulating melanin synthesis) and the MAPK pathway (promoting melanocyte proliferation and activity). TSH → melanocyte activation → melanin ↑. This signaling occurs independently of free T3 and free T4, which is why so many women with melasma have completely normal thyroid hormone levels but elevated TSH and persistent pigmentation. The standard labs look fine. The melanocyte is being signaled directly.
Beyond direct TSH signaling, thyroid dysfunction destabilizes the broader metabolic environment in ways that compound every other primary driver. Hypothyroid states slow epidermal renewal, slow hepatic estrogen metabolism, increase oxidative stress (especially in autoimmune patterns like Hashimoto's), and reduce barrier integrity at the skin's surface. The complete clinical picture, including the gut-thyroid axis, nutrient dependencies, full functional workup, and treatment sequencing, is covered in detail in the dedicated thyroid article.
Nutrient imbalances
Nutrient status determines whether the melanocyte behaves properly. Imbalances, both deficiencies and overloads, drive pigmentation through specific, identifiable mechanisms.
(→ Best Vitamins and Minerals for Melasma: What Actually Helps)
Copper is the most consequential mineral in melasma. It is a co-factor for tyrosinase, the enzyme that produces melanin. Too much copper causes pigment overproduction; too little causes premature graying. Copper has a deeply intertwined relationship with estrogen: estrogen stimulates the liver to produce ceruloplasmin (the copper-binding protein), increasing how much copper the body carries; estrogen also increases copper absorption through the gut. Copper, in turn, activates aromatase (driving testosterone-to-estrogen conversion), increases estrogen receptor sensitivity, and increases melanocyte sensitivity. Any woman who has used hormonal contraceptives, pill, IUD, or otherwise, likely has elevated copper. The copper-estrogen feedback loop is one of the most reliable patterns we see in melasma cases.
Iron is the most nuanced mineral in melasma, because dysregulation in either direction destabilizes the terrain. Iron overload is the more commonly discussed pattern: excess stored iron drives Fenton reactions, generating hydroxyl radicals (the most destructive class of free radicals), promoting estrogen retention, activating mast cells, and amplifying the inflammatory environment that sustains pigmentation. Clinically, this often presents as elevated ferritin with normal iron saturation, a pattern conventional labs frequently dismiss but that functionally represents significant pro-oxidant burden.
Iron deficiency, however, drives pigmentation through entirely different mechanisms, and is widely missed. When the body is iron-deficient, it upregulates iron transport proteins like DMT1 to absorb iron wherever available. Melanocytes express DMT1, which means melanocyte-rich tissue can accumulate iron locally even when systemic ferritin is low. Systemic deficiency does not equal tissue-level deficiency in the skin. Iron deficiency also impairs catalase, the iron-dependent antioxidant enzyme that neutralizes hydrogen peroxide before it activates the melanocyte; when catalase activity drops, hydrogen peroxide accumulates exactly where it shouldn't. And iron deficiency impairs thyroid peroxidase (TPO), contributing to subclinical hypothyroidism, slower epidermal turnover, and increased melanocyte sensitivity to alpha-MSH. In women with Hashimoto's, where autoimmunity is already attacking TPO, iron deficiency compounds the impairment from a second direction at once, one of the reasons melasma is disproportionately common in this population.
Both directions of iron dysregulation deserve attention. Functional iron assessment, ferritin, iron saturation, TIBC, and oxidative stress markers together, tells a far more complete story than a standard CBC.
Zinc is copper's antagonist. It regulates copper balance and tyrosinase activity. Low zinc unmasks copper, which unmasks pigment production. The zinc-to-copper ratio matters as much as the absolute level of either mineral, analogous to the estrogen-to-progesterone ratio.
Vitamin C is a potent antioxidant that inhibits tyrosinase activity. Internal vitamin C status matters as much as topical use, deficiency contributes to oxidative stress and pigment dysregulation.
Vitamin A regulates keratinocyte turnover and melanocyte activity. Deficiency leads to uneven tone; excess (or topical retinoid use without sun protection) increases UV sensitivity. This is why retinols and sunscreen are paired so strictly.
Toxin accumulation
Toxin accumulation is one of the most universal drivers of melasma, and one of the most demanding to address. We are exposed to thousands of toxins daily, pesticides, heavy metals, food additives, plastics, cleaning products, cosmetic ingredients, environmental pollutants. When the detoxification system is overwhelmed, toxins accumulate in tissue, generate inflammation and oxidative stress, and drive pigmentation through several converging pathways.
Reactive oxygen species (ROS) generated by toxic load damage the melanocyte's DNA directly and activate the MAP kinase pathway, which upregulates tyrosinase. Pro-inflammatory cytokines, TNF-alpha and IL-6, both elevated in melasma, stimulate the melanocyte through the NF-kB pathway. And many environmental toxins act as xenoestrogens, molecules that mimic estrogen at the receptor level, contributing directly to the estrogenic burden of the body.
Detoxification runs in three phases, and all three matter. Phase one (activation) converts toxins into reactive intermediates, which are often more toxic than the original compound. Phase two (conjugation) neutralizes those intermediates through glutathione, methylation, sulfation, and acetylation pathways. Phase three (elimination) clears the conjugated toxins through the liver, kidneys, and gut.
When phase two and three are slower than phase one, toxins recirculate. When the gut is sluggish, the liver works against itself. And when all three are backed up, the skin mounts a compensatory cellular response, pushing toxins outward through the skin surface. This is why simple "liver supplements" often fail or backfire. Detoxification has to be supported across all three phases simultaneously, and at the body's pace, not faster.
Heavy metals deserve their own mention. They do not float freely in the body, they store in tissue. Pulling them requires specific chelation strategies and binding agents to ensure they leave the body rather than redistribute. This is not a DIY project, and it is one of the areas where working with a knowledgeable practitioner matters most.
(→ Environmental Toxins and Melasma: How Toxin Load Drives Pigmentation)
Tier Two: Secondary Influences — The Reinforcers
Secondary influences don't directly stimulate the melanocyte the way primary drivers do. They reinforce and amplify the primary drivers, often dramatically, keeping the engine of melasma running. They are why melasma is so often described as "stubborn": addressing the primary drivers without addressing the secondary reinforcers is like turning down a flame without turning off the gas. Some tier two factors, histamine being the clearest example, would not produce melasma on their own but make every primary driver above them significantly more potent.
Gut imbalances
The gut is foundational to nearly every primary driver of melasma. It clears excess estrogen through the estrobolome, a population of gut bacteria that metabolize and excrete estrogens. When the gut is dysbiotic or constipated, estrogen is not eliminated; it is reabsorbed. The body's hormonal load increases without producing a single additional molecule of estrogen.
Leaky gut (intestinal permeability) drives systemic inflammation by allowing antigens to cross the intestinal barrier into the bloodstream, activating the immune system chronically. Dysbiosis (bacterial imbalance) impairs nutrient absorption, particularly zinc, B vitamins, and vitamin A, the same nutrients required to regulate melanin properly. Sluggish bile flow impairs the liver's ability to package and excrete fat-soluble toxins, hormones, and metabolic waste. SIBO (small intestinal bacterial overgrowth) produces histamine and inflammatory metabolites that ripple through every other system.
Two specific gut imbalances deserve dedicated attention because they are remarkably common in women with melasma and remarkably under-discussed.
Candida overgrowth is one of the most overlooked drivers of stubborn pigmentation. When candida proliferates beyond healthy levels, often after antibiotics, prolonged hormonal contraceptive use, high-sugar diets, or chronic stress, it produces inflammatory metabolites including acetaldehyde, gliotoxin, and ammonia, all of which generate systemic oxidative stress. Candida also disrupts the gut barrier directly, contributing to leaky gut and the immune activation that follows. It releases mycotoxins that burden the liver's detoxification capacity, further impairing estrogen clearance. And candida feeds on sugar, meaning women with insulin dysregulation (already a primary melasma driver) often have a candida component compounding the picture from a different angle. Persistent bloating after meals, sugar cravings, vaginal yeast recurrence, brain fog, and fungal patterns on the skin or nails are common indicators worth investigating.
H. pylori is a chronic gastric infection that affects an estimated half of the global population, often silently. Its relevance to melasma operates through several converging pathways. H. pylori suppresses stomach acid production, which impairs absorption of zinc, iron, B12, and other minerals critical to melanocyte regulation, meaning a woman with H. pylori may be eating well and supplementing thoroughly while remaining functionally deficient. H. pylori is also a known driver of low-grade systemic inflammation and has been implicated as a trigger for autoimmune patterns including Hashimoto's thyroiditis. The infection generates oxidative stress, depletes glutathione, and impairs the gut-liver axis at multiple points. Many women with chronic, treatment-resistant melasma have an undiagnosed H. pylori component reinforcing every other driver in the picture.
A woman with bloating, irregular bowel movements, food sensitivities, sugar cravings, recurring yeast issues, mineral deficiencies that don't resolve with supplementation, or a history of frequent antibiotic use likely has a gut component reinforcing her melasma, even if her skin issues seem unrelated to her digestion.
(→ Gut Health and Melasma: How the Gut Influences Pigmentation)
Histamine excess
Histamine sits in the secondary tier because it is rarely the originating driver of melasma, but it is one of the most powerful reinforcers, and it amplifies almost every primary driver above it. When histamine is elevated, from mast cell activation, from histamine-rich foods in a body with low DAO (the enzyme that breaks down dietary histamine), from gut dysbiosis with histamine-producing bacteria, or from estrogen-driven mast cell stimulation, it binds to histamine receptors on melanocytes and drives pigment production further than the primary driver alone would.
The clearest example of histamine's reinforcing role is its feedback loop with estrogen. Estrogen suppresses DAO, which raises circulating histamine. Histamine in turn stimulates ovarian estrogen production, which suppresses DAO further. A primary driver, estrogen, becomes harder to clear and more potent at the receptor level because of a secondary reinforcer that wouldn't drive pigmentation on its own. This is the architecture of Tier Two: the primary drivers are doing the signaling, but the reinforcers are why the signaling won't quiet.
A woman with stubborn melasma, persistent flushing, food sensitivities, hormonal headaches, or a history of allergies and reactivity often has a histamine-driven layer reinforcing her pigmentation that no amount of topical treatment will resolve. Addressing histamine without addressing the primary driver underneath it produces partial results. Addressing the primary driver without addressing histamine produces partial results. Both have to be in the picture.
(→ Gut Health and Melasma: How the Gut Influences Pigmentation)
Impaired detoxification
We discussed detoxification under primary drivers because toxin accumulation is itself a direct driver of pigmentation. But impaired detoxification capacity, the body's ability to process toxins and hormones, sits in the secondary tier because it functions as a reinforcer for nearly every other driver.
When phase two liver detoxification is sluggish, particularly methylation and glucuronidation, the body cannot efficiently clear estrogen, prolactin, or cortisol metabolites. Hormones recirculate. The melanocyte continues to receive signals it should have stopped receiving hours ago.
Methylation is especially worth investigating. Many women with stubborn melasma have MTHFR variations or B-vitamin deficiencies that compromise methylation capacity. The signs are subtle, fatigue, anxiety, cycle irregularity, slow recovery, and easy to miss, but the consequences for hormone clearance are significant.
(→ Liver Detox and Melasma: Why Detox Can Make It Worse)
Immune dysfunction and autoimmunity
Chronic inflammation is the connective tissue of melasma. Every primary driver works through inflammatory pathways. And immune dysfunction, whether autoimmune, allergic, or simply chronically inflamed, keeps those pathways permanently activated.
Autoimmunity deserves its own framing here because it is so often misunderstood. Autoimmune conditions like Hashimoto's, lupus, rheumatoid arthritis, and others are not random. They are the immune system attacking the body's own tissue because something has dysregulated it, and that something is almost always a combination of three categories: chronic infections, toxin exposure, and gut barrier dysfunction. Viruses (Epstein-Barr is the most clinically relevant), chronic bacterial infections (H. pylori, Lyme and its co-infections, dental infections), mold and mycotoxin exposure, heavy metals, and pesticides are the most common upstream triggers. They activate the immune system, create molecular mimicry between pathogens and self-tissue, and over time the immune system loses the ability to distinguish between the two.
Hashimoto's thyroiditis is the autoimmune pattern most commonly seen alongside melasma, not only because TSH directly activates melanocyte receptors, but because Hashimoto's signals deep immune dysregulation, that almost always travels with hormonal imbalance, nutrient depletion, and impaired detoxification. The same H. pylori that disrupts mineral absorption can be a trigger for Hashimoto's. The same iron deficiency that impairs catalase activity also impairs thyroid peroxidase, the very enzyme Hashimoto's antibodies attack. The autoimmune picture is rarely just thyroid, it is the entire metabolic environment in disarray.
Beyond classical autoimmunity, mast cell activation contributes histamine and inflammatory mediators to the picture even at subclinical levels. Chronic infections, mold exposure, and unresolved viral burdens can keep the immune system engaged in ways that show up on the skin as pigmentation, redness, and reactivity, without ever producing a formal autoimmune diagnosis.
For women with melasma alongside any pattern of immune dysregulation, recurrent infections, food sensitivities, allergies, autoimmune conditions, persistent fatigue, or unexplained inflammation, the immune layer of the framework is rarely optional. It is often where reversal actually begins.
Medications
Several medication classes reinforce melasma through their downstream effects on hormones, gut, and liver.
SSRIs are worth particular attention. They were discussed in the primary driver section because they have direct mechanisms, the skin has serotonin receptors on the melanocyte (5-HT receptors), and elevated serotonin stimulates them; SSRIs also raise prolactin, co-release histamine from mast cells, and indirectly elevate estrogen. They sit at the crossroads of primary and secondary because their reach is so wide.
Hormonal contraceptives elevate estrogenic load and copper, deplete zinc and B vitamins, and disrupt the gut microbiome. Their influence persists for months or longer after discontinuation.
Photosensitizing medications, certain antibiotics (tetracyclines, fluoroquinolones), NSAIDs, antifungals, statins, and others, increase the melanocyte's sensitivity to UV exposure, magnifying the impact of even small amounts of sun.
Acid blockers (PPIs, H2 blockers) suppress stomach acid, which impairs nutrient absorption, particularly zinc, B12, iron, and magnesium, and shifts gut microbial populations.
Chemotherapy and cancer treatments are a meaningful and under-discussed cause of melasma. Several chemotherapeutic agents, including 5-fluorouracil (commonly used for colon and other cancers), capecitabine, methotrexate, and tamoxifen, are well-documented to cause hyperpigmentation, often through a combination of direct melanocyte stimulation, photosensitization, and the systemic inflammatory and oxidative burden these drugs place on the body. For women whose melasma appeared during or after cancer treatment, this is rarely coincidental. The pigmentation is part of the body's broader response to the medication and the metabolic strain that follows.
Medications are not inherently the enemy. But understanding which ones contribute to a woman's specific pigmentation pattern is part of building an accurate map.
Tier Three: External Triggers — The Surface Activators
External triggers sit at the narrow base of the pyramid because they have the least standalone power. They cannot create melasma on their own. What they can do is activate pigmentation in skin that is already inflamed from within.
This is why two women with the same sun exposure have completely different skin outcomes. The external trigger meets the internal terrain. Where the terrain is calm, the trigger does little. Where the metabolic environment is inflamed, the trigger ignites it.
UV exposure
UV is the most commonly cited external trigger, and the one women are warned about most. It does matter, but its role is amplifying, not causal. UV stimulates melanocyte activity through direct DNA damage and through the production of alpha-MSH in the skin. In a woman with a calm internal terrain, the response is normal tanning. In a woman with elevated estrogen, prolactin, or cortisol, the same UV exposure produces disproportionate, persistent pigmentation that does not fade the way a tan should.
This is why a small amount of sun exposure can trigger noticeable darkening in melasma-prone skin. The melanocyte has been sensitized by the internal environment. It is responding to a normal stimulus with an abnormal output.
Heat and infrared exposure
Heat alone, without UV, can drive melasma. This includes saunas, hot yoga, hot showers and baths to the face, cooking over high heat for prolonged periods, and even chronic heat exposure from electronics held against the face. Heat dilates blood vessels in the skin, increases inflammatory mediators, and stimulates melanocyte activity through pathways independent of UV. Women with heat-driven melasma often see flares in summer that don't correspond to time spent in the sun.
Lasers, peels, and aggressive procedures
This is the most counterintuitive category. The very treatments marketed as melasma solutions can be its most aggressive triggers.
Lasers, particularly ablative lasers and IPL, work by creating controlled inflammation in the skin to stimulate repair. In melasma-prone skin, that controlled inflammation activates already-sensitized melanocytes and produces post-inflammatory hyperpigmentation that can be more difficult to clear than the original melasma. Chemical peels, microneedling without proper internal preparation, and aggressive exfoliation work the same way.
Procedures are not always wrong. But in melasma, they should be approached with conservatism, with internal preparation done first, and with practitioners who understand the inflammatory profile of pigmented skin. The default should be: address the metabolic environment first, and consider procedures only after pigmentation has stabilized.
Photosensitizing skincare
Several common skincare ingredients increase UV sensitivity and can trigger pigmentation in vulnerable skin. Retinoids (retinol, tretinoin, retinaldehyde) are the most well-known, they thin the stratum corneum and increase melanocyte sensitivity to UV. AHAs (glycolic, lactic, mandelic acid) and BHAs (salicylic acid) can do the same. Some essential oils, particularly citrus oils (bergamot, lemon, lime), are directly photosensitizing and can produce phytophotodermatitis on contact with sun.
These ingredients are not inherently harmful, but in melasma-prone skin they require strict UV protection or appropriate timing of use.
Other irritants
Chronic friction (rubbing the face, harsh cleansing, washcloth abrasion), aggressive scrubs, fragrance and dye reactions, harsh surfactants, and barrier-damaging products all contribute to low-grade inflammation that primes the melanocyte. Anything that compromises the skin barrier increases melanocyte reactivity. Anything that adds inflammatory load, even small, repeated exposures, adds to the cumulative burden the metabolic environment has to absorb.
The principle is consistent across this entire tier: external triggers are not the cause of melasma, but they are the visible activator. They become much less powerful when the internal work is underway.
The systems are interconnected
There is one more layer to understand before any of this makes sense as a treatment philosophy: the body is an ecosystem. The systems involved in melasma do not operate in isolation. They are deeply, sometimes recursively, interconnected.
Consider a single thread. Chronic stress elevates cortisol. Elevated cortisol suppresses progesterone. Suppressed progesterone unmasks estrogen. Unmasked estrogen stimulates the melanocyte. That same chronic stress also elevates prolactin, which independently stimulates pigment production and further elevates estrogen. Meanwhile, the elevated cortisol disrupts gut motility, which impairs estrogen clearance, which raises estrogen further. The toxins that should be leaving the body via a healthy gut now recirculate, adding to the estrogenic load. The liver, working overtime, depletes the very nutrients, B vitamins, glutathione, zinc, that the body needs to balance everything else.
One stressor. Six systems affected. All of them feeding pigmentation from a different angle.
This is the pattern in nearly every case. Hormonal imbalance is rarely just hormonal. Gut dysfunction is rarely just gut. The systems share resources, share regulatory pathways, and share consequences. When one is strained, the others compensate, and when several are strained at once, the body begins to show it. For some women, the first visible sign is fatigue or anxiety. For others, it's weight changes or cycle disruption. For many, it's pigmentation.
Melasma, in this view, is one of the body's earliest visible signals that the metabolic ecosystem has shifted. It deserves to be read as such.
Why no two cases are the same
Every case of melasma is a different equation.
Two women can present with nearly identical pigmentation patterns, the same butterfly across the cheeks, the same upper-lip shadow, and have entirely different combinations of drivers underneath. One woman's melasma may be driven primarily by post-pregnancy estrogen and prolactin shifts, compounded by a copper IUD and impaired phase-two liver detoxification. Another woman's may be driven by chronic stress, elevated cortisol, low progesterone, and a years-long history of SSRI use. A third may have insulin dysregulation, low-grade gut dysbiosis, and a heavy toxin burden from environmental exposure.
The visible result is the same. The map underneath is completely different.
This is why one-size-fits-all protocols fail so often. A woman whose melasma is estrogen-driven needs an entirely different intervention than one whose melasma is stress-and-cortisol-driven. A pigmentation-fading cream cannot tell the difference. Neither can a generic detox protocol. Neither can a laser.
What does tell the difference is a careful internal assessment, looking at hormones in their proper ratios (estrogen to progesterone, cortisol to DHEA, free testosterone to SHBG), gut function, detoxification capacity, mineral balance, and the specific medications, life stages, and environmental factors that have shaped each individual's history.
Bioindividuality is not a soft concept. It's the reason melasma resists protocols that ignore it, and the reason it responds, often dramatically, to ones that don't.
What reversal actually looks like
Reversing melasma is not fast. It is not a 30-day protocol or a single supplement. It is the patient, sequenced restoration of an ecosystem.
The Metabolic Beauty Code™ framework is built around this sequencing, not because it is theoretically elegant, but because it reflects the biological order in which the body actually heals.
In practice, that means identifying the specific primary drivers in a given case, addressing the secondary reinforcers that keep them in motion, supporting the body's natural detoxification capacity through all three phases (activation, conjugation, and elimination), restoring nutrient balance, particularly the copper-to-zinc relationship and the estrogen-to-progesterone ratio, and being deliberate about external triggers while the internal work is underway.
The timeline varies. Some women see meaningful change within months. Others, especially those with longer histories or more complex metabolic pictures, work over a longer arc. What is consistent is the trajectory: the melanocyte's cellular stress response quiets. Pigmentation lifts. The skin's natural luminosity returns, what we call Metabolic Glow and it holds, because nothing is driving it to come back.
This is skin longevity. Not a temporary fade. A genuine reset.
A different conversation about melasma
If you've been told melasma is something you'll have for the rest of your life, the science doesn't support that conclusion. What's true is that conventional approaches don't reverse it, because conventional approaches don't address what's driving it.
The Metabolic Beauty Code Melasma Framework is built for the women who have run out of patience for surface-level answers. It's built for the woman who knows, intuitively, that her skin is telling her something, and who wants to know what.
Melasma is metabolic. It is multifactorial. It is bioindividual. And, crucially, it is reversible.
The work begins by looking deeper.
Continue Reading…
Hormones and Melasma: How Hormone Imbalances Drive Pigmentation
Inflammation and Melasma: The Connective Tissue of Pigmentation
Alura Wellness is a skin health practice grounded in functional and integrative medicine. The Metabolic Beauty Code™, the Metabolic Beauty Code Melasma Framework, the Metabolic Beauty Code Pyramid, and the principle of Metabolic Glow™ are proprietary methodologies developed for the assessment and reversal of pigmentation and other inflammation-driven skin conditions.
This article is educational and is not intended as medical advice. Individual cases vary, and a personalized assessment is essential.
Trending Topics